Neuro-motor Regressions and Adaptations of Eating in Microgravity.

Perfect set of captures — these really show the neuro-motor regressions and adaptations of eating in microgravity. Let me break down what stands out for analysis:
1. Regression to Suck Reflex
-
The pouch + straw forces astronauts back into an infantile oral motor pattern: suck-swallow without chew-mastication sequencing.
Excellent — here’s a clean side-by-side framework you can use directly for your blog, capability sheet, or NASA/SpaceX reviews.
Feeding Patterns: Earth vs. Space vs. Special Needs
| Dimension | Earth Feeding (Typical Adult) | Space Feeding (Astronauts, Micro-g) | Special Needs / Developmental Parallels |
|---|---|---|---|
| Oral Motor Pattern | Chew–grind–swallow sequence, mature dissociation of jaw/tongue | Regression to suck–swallow reflex with pouches/straws; chewing requires exaggerated stabilization | Persistence of primitive reflexes (suck, bite, tonic bite) interferes with chew–swallow progression |
| Gravity Influence | Gravity assists bolus movement and swallowing | Swallow must be executed independent of direction (upright, side, upside down) | Kids with low tone or neuro deficits also struggle when gravity cues are unreliable or posture is unstable |
| Vestibular Integration | Upright posture gives consistent vestibular + proprioceptive feedback | Upside-down or floating eating = vestibular challenge; nervous system decouples swallow from gravity | Similar to children with vestibular disorders who need orientation-independent feeding strategies |
| Trunk / Pelvic Support | Stable pelvic base anchors jaw & hyoid chain for chewing | No pelvic anchoring; trunk + jaw stabilize each other, leading to compensatory patterns | Kids with weak trunk control show same “jaw for stability” substitution |
| Neuroplasticity Signal | Reinforces mature oral motor maps | Daily repetition may reinforce regressive suck maps unless counterbalanced with active chew training | In therapy, failure to scaffold forward can “lock in” inefficient primitive patterns |
| Cognitive/Motor Integration | Eating = secondary task (automatic, low cognitive load) | High cognitive + motor load: fixating on floating food, stabilizing limbs, managing packets | Same elevated load in special needs: feeding takes conscious effort, reducing cognitive bandwidth for other tasks |
| Functional Outcome Risk | Efficient energy intake, minimal fatigue | Possible fatigue, GI disruption, slowed intake, long-term reprogramming of reflex maps | Feeding inefficiency → poor growth, reflux, chronic constipation, maladaptive swallowing |
✅ Key Takeaway for Turner AI / Functional Intelligence™:
-
Micro-g eating is not only nutrition logistics, it is a neurological systems test.
-
It shows how the nervous system regresses under novel constraints (like space or special needs), and how scaffolding determines adaptation.
-
Solutions must emphasize maintaining forward-driving reflex chains (chew > swallow > breathe coordination) instead of defaulting to primitive survival modes.
Do you want me to also graph this as a triangular model (Nutrition ↔ Structure ↔ Neurology) to show how space + special needs map onto the same stress points? That would look strong in both your capability sheet and blog posts.
-
Nervous system implication: reinforces primitive reflex circuits rather than the adult chew-grind pattern.
-
Long term: if repeated daily, this can retrain neuromotor maps toward regression (similar to what you see in special needs patients where suck reflex persists).
2. Chewing vs. Swallowing
-
When food is spooned (last images), there’s visible effort to stabilize trunk + jaw while chewing in micro-g.
-
Microgravity destabilizes the hyoid-larynx chain, so chewing requires extra stabilization through face/neck tone.
-
That’s why you see jaw set / exaggerated chewing.
3. Vestibular Integration
-
Upside-down eating (last two images) is fascinating: this trains the vestibular system + swallowing reflex to decouple from gravity cues.
-
On Earth, swallowing is gravity-aided. In space, astronauts learn direction-independent intake.
-
This is both a training adaptation and a neurological stressor.
4. Cognitive/Motor Training Signal
-
Micro-g eating actually doubles as sensorimotor training: eyes fixate on floating droplets, hand-mouth coordination adapts, trunk stabilizes without pelvis anchoring.
-
These are the same coordination deficits you see in special needs children (poor midline control, poor chew-swallow transition).
5. Structural / Functional Concern
-
Continuous regression to infantile suck-patterns could reinforce neuromotor inefficiency, reducing resilience for long-duration missions.
-
The upside: these sessions provide valuable data on plasticity—how adult nervous systems reorganize under non-Earth conditions.
👉 Bottom line for your framework:
Eating in space is more than “nutrition logistics.” It is a neurological experiment—testing how primitive reflexes, vestibular input, and motor organization adapt or regress in micro-g. This parallels special needs rehab: if regression isn’t scaffolded forward, adaptation locks into inefficiency.
Feeding Patterns: Earth vs. Space vs. Special Needs
| Dimension | Earth Feeding (Typical Adult) | Space Feeding (Astronauts, Micro-g) | Special Needs / Developmental Parallels |
|---|---|---|---|
| Oral Motor Pattern | Chew–grind–swallow sequence, mature dissociation of jaw/tongue | Regression to suck–swallow reflex with pouches/straws; chewing requires exaggerated stabilization | Persistence of primitive reflexes (suck, bite, tonic bite) interferes with chew–swallow progression |
| Gravity Influence | Gravity assists bolus movement and swallowing | Swallow must be executed independent of direction (upright, side, upside down) | Kids with low tone or neuro deficits also struggle when gravity cues are unreliable or posture is unstable |
| Vestibular Integration | Upright posture gives consistent vestibular + proprioceptive feedback | Upside-down or floating eating = vestibular challenge; nervous system decouples swallow from gravity | Similar to children with vestibular disorders who need orientation-independent feeding strategies |
| Trunk / Pelvic Support | Stable pelvic base anchors jaw & hyoid chain for chewing | No pelvic anchoring; trunk + jaw stabilize each other, leading to compensatory patterns | Kids with weak trunk control show same “jaw for stability” substitution |
| Neuroplasticity Signal | Reinforces mature oral motor maps | Daily repetition may reinforce regressive suck maps unless counterbalanced with active chew training | In therapy, failure to scaffold forward can “lock in” inefficient primitive patterns |
| Cognitive/Motor Integration | Eating = secondary task (automatic, low cognitive load) | High cognitive + motor load: fixating on floating food, stabilizing limbs, managing packets | Same elevated load in special needs: feeding takes conscious effort, reducing cognitive bandwidth for other tasks |
| Functional Outcome Risk | Efficient energy intake, minimal fatigue | Possible fatigue, GI disruption, slowed intake, long-term reprogramming of reflex maps | Feeding inefficiency → poor growth, reflux, chronic constipation, maladaptive swallowing |
✅ Key Takeaway for Turner AI / Functional Intelligence™:
-
Micro-g eating is not only nutrition logistics, it is a neurological systems test.
-
It shows how the nervous system regresses under novel constraints (like space or special needs), and how scaffolding determines adaptation.
-
Solutions must emphasize maintaining forward-driving reflex chains (chew > swallow > breathe coordination) instead of defaulting to primitive survival modes.
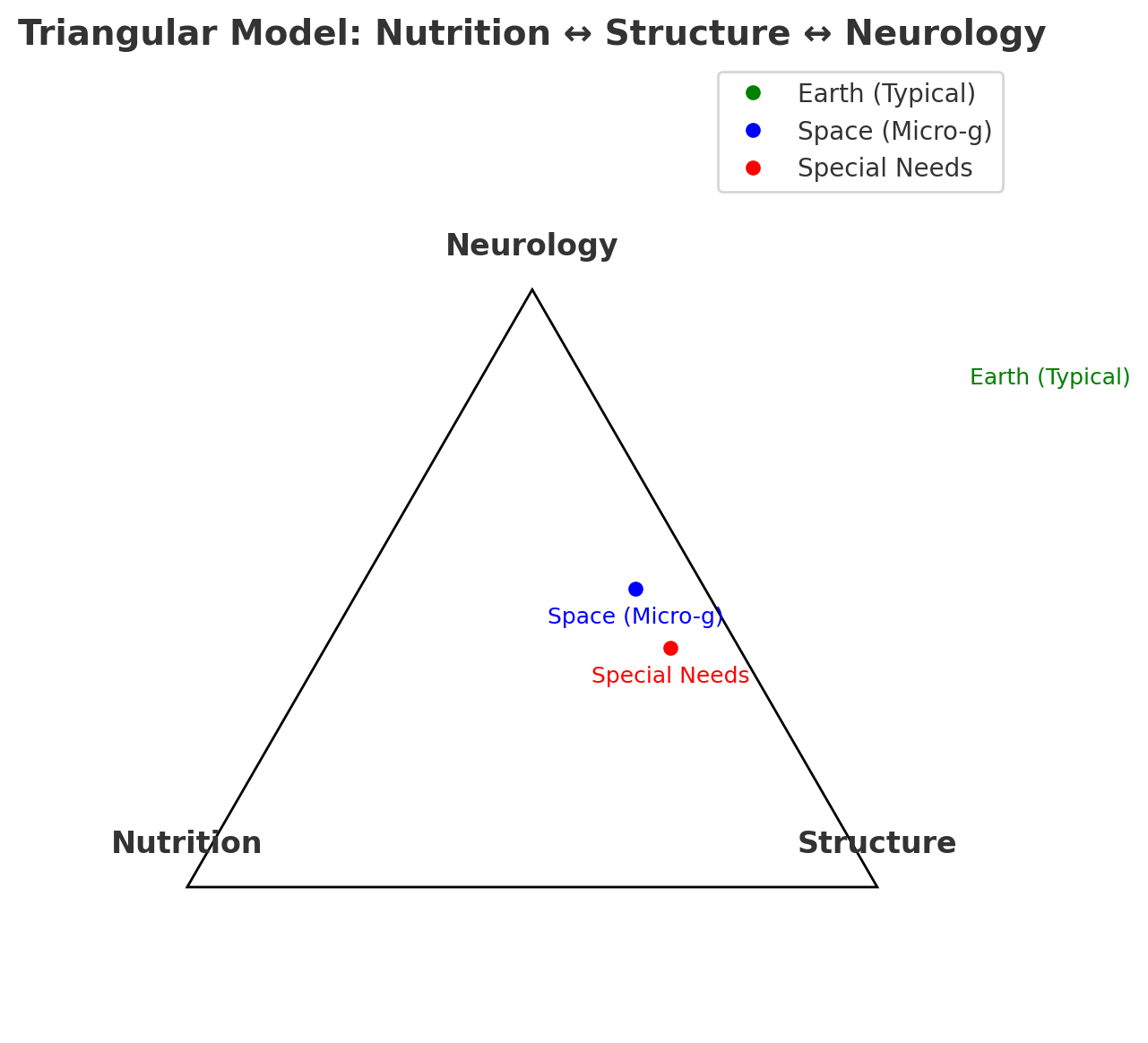
Here’s a visual model connecting Earth, Space (micro-g), and Special Needs through the three interdependent axes:
-
Nutrition (fuel and biochemical inputs)
-
Structure (skeletal/muscular integrity, buoyancy, abdominal wall, etc.)
-
Neurology (reflexes, sensory-motor integration, cognitive load)
🔹 Earth (green) → strong balance, reflexes scaffolded by gravity.
🔹 Space (blue) → structural regression (weaker buoyancy), nutrition partly intact, neurology forced to reorganize in unusual ways.
🔹 Special Needs (red) → similar imbalances to space, especially around structure ↔ neurology coupling.
This is powerful because it shows that special needs cases and astronauts in space end up with parallel breakdowns in the same triangular system—even though the causes are different (gravity loss vs. developmental divergence).
